Community hospitals seek right to do angioplasty
12/4/2005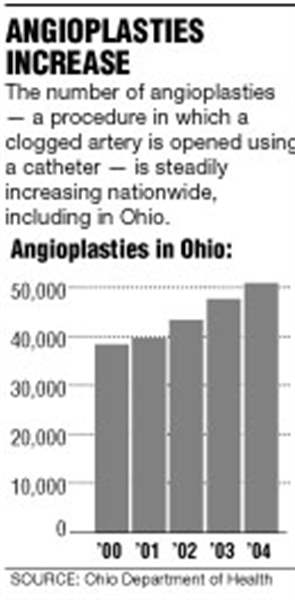

Angioplasty is among the most common - and lucrative - medical procedures done in big city hospitals, but a nationwide study involving six Ohio hospitals could make them a lot more common in small community or rural hospitals.
That possibility has divided cardiologists. Many feel the technology for angioplasty - a procedure in which a doctor reopens a clogged heart artery by inflating a tiny balloon in the artery - has improved so much that there's little risk involved. It makes sense to allow patients to get the procedure done close to their home instead of driving to a large hospital, they argue.
"The odds of having people needing emergency surgery, even in a large institution, are very low," said Dr. Philip Dorfman, president of the Ohio chapter of the American College of Cardiology. "If [the study] determines it to be safe and effective so patients don't need to travel, well, so be it."
Other cardiologists are skeptical. While the risk of complications is quite low, why take the chance at all, they counter. The real issue here, they say, is money: smaller hospitals wanting to get a piece of the money-making procedure.
"I am very concerned. This is a market-driven treatment strategy," said Dr. William Schafer, a Toledo cardiologist who performs angioplasties.
Hospital officials involved in the study urge skeptics to wait for the results before jumping to conclusions.
"We would never be looking at this if we didn't think our quality wasn't there," said Phil Ennen, chief executive officer of Community Hospitals and Wellness Centers in Bryan.
His hospital is one of the six in Ohio that has applied to be in the study (more are expected to apply) and the only one in northwest Ohio. The research project is being spearheaded by the Johns Hopkins School of Medicine.
Researchers there hope to enroll about 40 small hospitals from around the country and follow their outcomes for several years. They want to know if "elective" angioplasties, meaning those scheduled to be done on a nonemergency basis, can be performed safely at hospitals without on-site open-heart surgery capability. Typically, after an angioplasty is done a tiny piece of meshed metal known as a stent is inserted to keep the artery open.

Right now, the rule of thumb endorsed by many cardiologists is that only hospitals with open-heart surgery capability should attempt to do routine angioplasties or insert stents. That's the position endorsed by the American Heart Association and American College of Cardiology. The thinking is if something goes wrong, a patient could quickly be rushed to an operating room to correct it.
Doctors cite the possibility, for example, of the stent breaching a blood vessel, which may require surgery to repair.
Still, this standard isn't universally followed. Many states allow small hospitals without open-heart backup to perform routine angioplasties. Ohio requires a hospital to have open-heart backup before doing routine angioplasties, but state officials say they're willing to reconsider their rules depending on the outcome of the study.
So far Ohio, Alabama, Georgia, Illinois, Pennsylvania, and New Jersey have agreed to allow hospitals in their states to apply for the study. Hospitals in those states accepted into the study will be able to do routine angioplasties.
Mr. Ennen said his 70-bed hospital in Williams County just wants a chance to compete and offer residents in the area high-quality cardiac care.
"As time marches on, technology improves and the ability to do things at a community hospital becomes more of an option. Doing cardiac stents 10 or 15 years ago would have been a highly specialized service. Now, interventional cardiologists coming out of residency do these all the time," he said. "So if you can provide it safely at the community level, we should. And two, if we're going to maintain the specialties we have [in smaller towns and cities], then we have to be attractive to younger physicians coming out of residency."
Angioplasties and stents are clearly a growth area for hospitals. The American Heart Association said 650,000 angioplasties were performed in 2002, more than triple the amount in 1987. In Ohio, 51,103 angioplasties were done last year, one third more than in 2000. Heart disease is the No. 1 killer of men and women, so the field is expected to grow even more.
Hospitals are so keen on ensuring their access to angioplasty volume that many have entered into some creative arrangements with cardiologists. For example, four years ago, a group of cardiologists opened a facility on the campus of St. Vincent Mercy Medical Center in Toledo to do low-risk heart catheterizations, a procedure in which a cardiologist inserts a thin tube through a blood vessel in the arm or leg area and slides it into the heart. A dye is then injected to look for blockages.
If an angioplasty is needed, the patient can then be transported to any hospital that performs them.
The setup financially benefits doctors because physicians can reap all of the revenue. In most traditional catheterization programs, physicians share revenue with hospitals.
Under the arrangement at St. Vincent, physicians pocket all of it. St. Vincent would make money by offering to do any angioplasty or stents on patients where blockages were found. Toledo Hospital opened a catheterization lab with a similar financial setup last week.
Dr. Daniel Cassavar, director of the catheterization lab and invasive services at Toledo Hospital, said he welcomes the Johns Hopkins-led study. He said supporters of smaller hospitals doing angioplasty are right to say the risk of performing angioplasties today is extremely low using modern technology.
Still, he's hesitant about recommending one of his patients get an angioplasty done at a hospital without open-heart surgery backup.
"It doesn't mean it can't be done [at smaller hospitals]. But if you ask me to give my family or my patient the best chance, at the present time, I'd want them at a [large] center," he said. "But that's why we do these studies."
Contact Luke Shockman at: lshockman@theblade.com or 419-724-6084.